
Disparities in Care Emerge in Resource-Limited Contexts
Evidence suggests significant obstacles in providing timely and effective treatments for ST-segment elevation myocardial infarction (STEMI) in areas with limited resources. These challenges stem from a fractured healthcare landscape where access to different levels of care, from hospitals capable of simple drug administration to those equipped for complex interventions, creates stark differences in patient outcomes.
A prospective observational study tracking 300 patients highlights the variability in medical contact points before reaching a study site. Hospitals are categorized by their capabilities: Lysis Capable Hospitals (LCH), PCI/Lysis Capable Hospitals (PLCH), and Non-Lysis Capable Hospitals (NLCH). The study collected data on interventions received at first and second medical contacts, alongside reasons for not receiving recommended care, indicating systemic inefficiencies.
Reperfusion Strategies: A Divide in Practice
The established gold standard for STEMI patients, primary percutaneous coronary intervention (PPCI), is not universally accessible. Studies from regions like Tamil Nadu, India, reveal a program that prioritizes PPCI for patients located near designated hub hospitals with catheterisation laboratories. This inherently creates a disparity, leaving those further afield to rely on alternative reperfusion strategies.
A secondary analysis of the Acute Coronary Syndrome Quality Improvement in Kerala (ACS QUIK) Trial sheds light on this divide. While PPCI remains the recommended approach, the analysis compared non-PPCI (nPPCI) to PPCI strategies.
| Strategy | Patients (Propensity-Matched) | Key Findings |
|---|---|---|
| nPPCI | n=1266 | Similar transfer rates to PPCI. Longer door-to-balloon time once at PCI-capable hospital (108 minutes). |
| PPCI | n=1266 | In-hospital and 30-day Major Adverse Cardiovascular Events (MACE) were similar to nPPCI. |
This suggests that while in-hospital and short-term adverse events might be comparable between strategies, the process and timing of care, particularly for nPPCI patients needing transfer, are markedly different.
The Shadow of Resource Constraints
The core issue appears to be the availability and accessibility of advanced interventions. The fragmented nature of healthcare systems in resource-limited settings is a persistent theme. This includes disparities in hospital infrastructure, such as the presence of catheterisation laboratories, and the administration of critical early treatments like fibrinolytic agents.
The prompt delivery of reperfusion therapy, whether via drugs or mechanical intervention, is paramount in STEMI management. When this delivery is hampered by distance, logistical hurdles, or a lack of equipped facilities, patient prognosis suffers.
Background:
ST-segment elevation myocardial infarction (STEMI) is a critical form of heart attack requiring immediate intervention to restore blood flow to the heart muscle. In regions with robust healthcare infrastructure, Primary Percutaneous Coronary Intervention (PPCI), a procedure to open blocked arteries with a balloon and stent, is the preferred method. When PPCI is not immediately feasible, fibrinolysis (clot-busting drugs) is often used as a first step, especially in more remote areas. However, the effectiveness and timely administration of both these treatments are heavily dependent on the availability of specialized medical personnel and equipment, which are often scarce in low- and middle-income countries. Research in these areas focuses on adapting treatment protocols and improving logistical chains to overcome these limitations and reduce mortality.
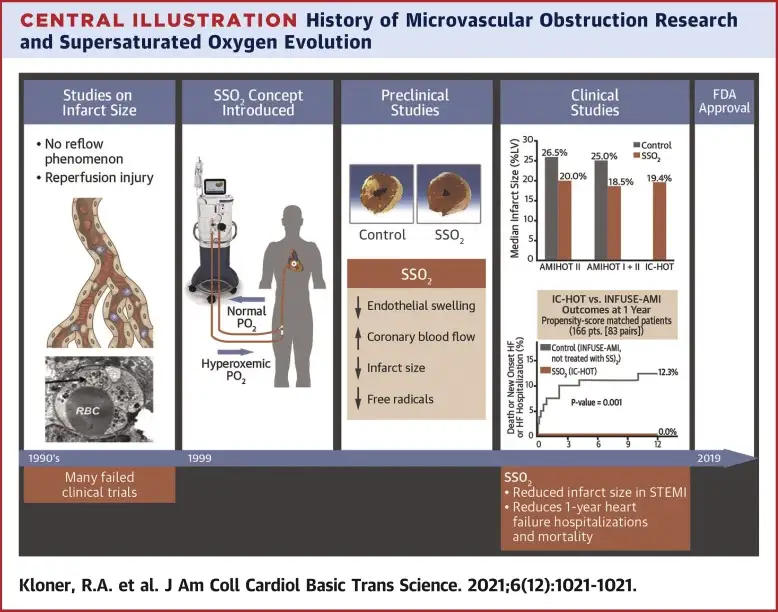
One area of investigation, though not directly comparing reperfusion strategies in the provided articles, explores novel cardioprotective agents like supersaturated oxygen delivery. This research aims to reduce infarct size and protect heart muscle during acute events, potentially offering adjunctive benefits regardless of the primary reperfusion method used. However, the immediate challenge in resource-limited settings remains the foundational access to timely and appropriate reperfusion itself.